
This post is about HIV prevention education. I’ll also have a few words to say about PrEP and how it relates to prevention education.
I hope that the recent National Conference on HIV Prevention, which considered several approaches to HIV prevention will mark a new beginning in prevention education.
The reduction in the spread of the epidemic in the late 1980s among groups of gay men in the US occurred mostly because so many men adopted safer sex practices, including condom use. This means that, in principle, prevention education can work.
It is a proof of concept, although admittedly without application to those who have no control over prevention intervention involving condom use by their male partners.
If prevention education has not worked so well in the US since that time, it is because there has not been much of it. What little there has been has generally not been appropriately targeted to those specific communities at particular risk. This is despite the fact that we have known since the late 1980s into which communities the epidemic was moving. So, again I hope that the recent conference means that we can expect improved, properly targeted prevention education efforts directed to where they are most needed.<
Was the success of prevention education in the mid to late 1980s among gay men a peculiar circumstance that has no relevance to others at risk?
I don’t think this is the case. It is not the only example of the success of prevention education. In a totally different situation, the number of HIV infections in Uganda fell in the 1990s. This coincided with the introduction of an intensive prevention education initiative.
Of course the characteristics of the epidemic in the US and Uganda are enormously different; the major means of transmission in Uganda is through heterosexual sexual contact and using this example certainly does not mean that those prevention education measures adopted in Uganda would be appropriate in the US. The example is an illustration that prevention education can work.
With these very different examples we can safely say that in principle, HIV prevention education can be effective.
In the US, in the early years of the epidemic, we had the horrible constant reminder of what we were facing in the frequent deaths of our friends and patients, an experience that younger people are now spared, at least on a daily basis. It seems absolutely reasonable to accept that these terrible reminders of what HIV infection could do contributed to the success of safer sex campaigns. Of course there are other differences today, not the least of which is that we have the great benefit of the availability of antiviral drugs.
The disease is viewed in a different way now, from something that seemed to be uniformly fatal to a “chronic manageable disease”. I have put the term in quotes because it is a misleading message put out by many health departments, and the Centers for Disease Control (CDC), as an explanation why HIV tests should be as routine as having your blood pressure taken. While there is of course every reason to test for HIV as widely as possible, it’s my opinion that comparing HIV disease to conditions like high blood pressure to promote testing can have a negative effect on prevention education.
Chronic, so called manageable diseases are in fact not all the same. Some are manageable with great difficulty and sometimes for not very long. The means used to manage the disease may themselves not be free from problems.
HIV disease has, without question, been transformed by the availability of antiviral drugs. But it still requires lifelong regular medical supervision, adherence to treatment regimens and, for some, dealing with severe adverse responses to the medicines. Then there is frequent stigmatization, difficulties in finding care, problems with employment, alienation of family, and a multitude of other difficulties that many people with HIV must face. No, HIV disease is not like having high blood pressure, diabetes or asthma, as the CDC would have one believe.
Despite this, it is possible that the message that HIV disease is now not so serious that is implicit in the reassuring description of the disease as a chronic manageable one, may have lessened the fear of becoming infected in some individuals. This is also a possible effect of some advertisements for antiviral drugs that suggest that taking them will transform one into a mountain climber.
But these and other obstacles to effective prevention education programs should be taken into account when designing new strategies. They can be overcome if there is a will and funding to mount large-scale properly targeted prevention education campaigns.
The most effective prevention education efforts can only have a chance of success if they involve the affected communities at every level. With a need for highly targeted prevention education material, various community groups are best able to craft the messages that are best suited to their needs, if given adequate resources.
The first proposal to use condoms in 1982, came from individuals under threat themselves, not from any organization, and certainly not from a government where the President at that time was unable to even mention the word AIDS or later, one who supported abstinence-only programs.
In 1982, despite the opposition of organized community groups, I with two of my patients, Michael Callen and Richard Berkowitz, were able to disseminate a booklet suggesting the use of condoms. This endeavour was made possible, not by a foundation or any other organization, but by an individual, Randall Klose who provided the funds. Few probably remember Randy Klose, but many should know about him and what he made possible. Even the foundation that I had incorporated, the AIDS Medical Foundation (which became Amfar) found the explicit words of the booklet a danger to fundraising, and refused financial support. They did help however, by providing fiscal sponsorship of Randy’s donation.
This was a community triumph. It arose from affected people themselves, who were not about to wait for some benevolent authority to introduce some way to prevent getting this disease.
When I started this post I pointed to the success of prevention education among groups of gay men in the mid to late 1980s. I had to say groups because just as cases were declining in white gay men they were increasing in African-American men.
The neglect of prevention education that is properly targeted to those at risk that is culturally-sensitive and persistently delivered is demonstrated in the most awful way by the current disaster in many African-American communities.
I, as many of us, have been following demographic trends of the epidemic since its start. The advance of this disease into African-American communities became quite apparent in the late 1980s, visible to all who cared to look at surveillance data. By 1993 the percent of diagnoses in African-Americans started to exceed that in white Americans. Certainly by 1990, we could have had no better evidence to target a group in great need of prevention education, yet “America Responds to AIDS” was the best we could come up with. For those who did not see this program, it was a vacuous untargeted waste of money and time and an indication of ineptitude or indifference on the part of authorities whose task it was to protect us.
Take a look at this picture that tells a horrible story that words cannot match.
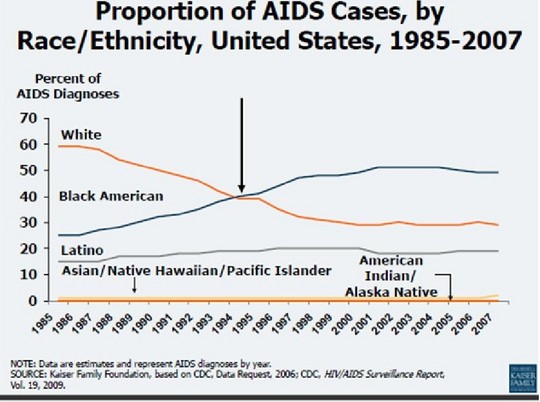
This represents a tragedy that has been developing in full view for more than twenty years. We knew as early as 1987, and certainly in 1990, that without intervention a preventable disease would inexorably move into African-American communities. This picture tells us exactly how America responded to AIDS.
In February, 2009 he noted that these “shocking statistics would be tragic anywhere but are particularly inexcusable in a wealthy country such as the United States”
His complete statement can be seen here:
http://www3.niaid.nih.gov/news/newsreleases/2009/BAAID_09.htm
But this is only one of endless comments by authorities on a tragedy that was developing before their eyes for twenty years. The same might be said about the many comments on the dire condition in Washington DC.
It is not only the federal AIDS leadership that failed to respond to warning signals flashing brightly right in front of them. In the early days of the epidemic there was a vigorous and exemplary community activist response. This was a terrific example of people dealing with a deadly disease taking action on their own behalf, fighting for the best medical and scientific response and against the shameful stigmatization of HIV infected individuals.
The flowering of AIDS activism in the late 1980s and early 1990s achieved a great deal. All people dealing with serious illness have benefitted from the precedent that was set. Yet, in recognizing this achievement, we must also wonder why many of these experienced advocates, who no doubt were aware of the demographic trends shown above, seemed generally less willing to at least try to avert the disaster threatening their fellow citizens? Of course some tried, and maybe were overwhelmed by massive indifference.
Whatever the reasons, the advocacy of US activists abroad, particularly in Southern Africa, proved to be more effective than anything they were able to achieve in their own country for their fellow African American citizens.
There are also other groups where AIDS has been, and continues to be a growing problem, but have been relatively neglected.
To conclude this post I want to explain why HIV prevention education must be closely linked with the promotion of studies on PrEP.
This will also be a response to some comments made following my last post on PrEP, particularly those of Anna Forbes of the Global Campaign for Microbicides (GCM). If you click on this link you will find several papers on ethical issues associated with prevention trials, as well as the links Anna Forbes provided in her response, to in-depth analyses of previous problems in PrEP trials in Cambodia and Cameroon.
I should say that Anna Forbes’ presentation at the CHAMP teleconference was extremely good; she made it quite clear that PrEP was not intended to be a replacement for current recommendations which include the use of condoms.
What I have written above about my involvement with prevention education ever since our booklet “How to have sex in an epidemic: one approach” was written in 1982 should explain the position from which I wrote my last POZ blog post, and why I responded as I did, particularly to the CHAMP flyer.
When I read the flyer I feared that by failing to state that PrEP was not a replacement for current prevention approaches, the interpretation made by some might have been that prevention education is ineffective and that therefore a new prevention strategy was needed. More people probably saw the flyer or eblasts than participated in the teleconference where the issue was clarified.
It is of course true, as one person stated, that a flyer cannot contain all details. But surely a statement that PrEP is not intended to replace current prevention recommendations including condom use should have been there.
Most of this post has been a defence of HIV prevention education, arguing that it would be quite wrong to conclude that in principle, it is ineffective. The failing has been in the efforts of those responsible for it, a lack of interest or maybe just a belief that the effort would be useless. As for funding, while the changes shown in the above illustration were steadily progressing in full view, “America Responds to AIDS” was on every TV set in the country. That must have cost many millions.
As with almost everything in HIV medicine, a one-size-fits-all approach seems to be the norm. It’s certainly cheaper to deal with populations rather than customize responses to fit the needs of individuals. Treatment recommendations are made without concern for individual differences in the rate of disease progression. At the very least, North America and Europe can afford the expense of individualizing treatment for HIV, as is typical for most other life-threatening conditions.
In the same way there are differences in prevention needs in different communities and differences within these communities. These differences are reflected in differences in what is hoped for from PrEP.
For some women (and some men) PrEP may represent the most practical, though as yet unproven, way to avoid HIV infection.
For others, both men and women, it may represent an added layer of protection to condom use or other risk reduction measures.
Some may hope that it will provide a safe means to conceive.
Others evidently hope that it may represent a safe way to increase sexual intimacy for people with HIV by dispensing with condoms altogether, although I find it impossible to envisage how safety could ever be tested.
These are all very different situations; the stakeholders are indeed a diverse group.
Some need PrEP to remain uninfected while others want it, even though there is no insuperable obstacle to following current HIV prevention recommendations.
The power of men to protect themselves and their partner is the use of a condom. The only theoretical power available to a woman (apart from the female condom) is the power to say no. But I say theoretical power, because in real life there are many situations in which this power cannot be exercised.
It is clear that we need prevention interventions that are in the control of individuals who are the receptive partners in sexual intercourse. For these individuals, the study of PrEP is of the greatest importance.
As far as choosing to dispense with condoms is concerned, Swiss investigators have proposed a reasonable set of circumstances when this can be safely done. These circumstances will apply to very few. For others where infectivity is realistic, I can think of no way to determine if PrEP would provide a means to safely dispense with condoms.
Prevention education has been shown to work among men who have sex with men. And today in America, it is those men--Black, Hispanic, White, Native American, gay men of all ethnicities--who carry the greatest burden of this disease. So when new strategies are being explored, it is important that it is not even implied that prevention education is something that cannot work well enough, and therefore new prevention strategies are required. Presenting a new prevention strategy such as PrEP should be accompanied by an encouragement and strengthening of prevention education that we know can be effective.
As far as my comments on efficacy trials of PrEP are concerned, I believe there is a realistic possibility that a reliable and generalizable result on efficacy may unfortunately be impossible to obtain. There are added, but hopefully not insuperable potential problems, like adherence to PrEP and the risk of developing resistance. Now we also have the troubling news that pre-existing bone density issues among some African men may present a problem in the use of tenofovir as well as growing research indicating the demineralising effect of its long-term use.
It seems better to offer an unproven intervention that has something to support its use, with appropriate testing for infection and toxicity, rather than do nothing. Where conditions permit this, there is a case to be made for presenting this as an informed choice that individuals have every right to make on their own behalf. This would be the case where, in practice, there is no other intervention available. In the 1970s I prescribed antibiotics to patients as pre-exposure prophylaxis against gonorrhoea and syphilis, presenting adequate information and follow up testing. It was a choice I felt they had every right to make. Despite being chastised by my colleagues, I was able to prevent gonorrhoea and syphilis in some of my patients (of course I have no proof of this, but it is likely that infection was avoided). HIV infection however is quite a different matter, but still, with full information, making decisions on their own behalf remains the right of an individual. But we don’t yet have full information, and anti-retrovirals are available in many parts of the world. This is another reason to do what we can to complete efficacy trials of PrEP.
I certainly had no intention to discourage the study of PrEP; my interest was in strengthening and improving prevention education. This is something that must go hand in hand with the study and promotion of PrEP, not only in trials, where this is happening, but at a community level.




Comments
Comments