
A role for immune activation in a positive feedback system:
This continues my last post.
In summary; immune activation not only results from HIV infection, it can also promote further replication of HIV. HIV infection also increases susceptibility to some other infections which then can contribute to immune activation and further HIV replication.
HIV replicates more efficiently in activated immune system cells, and pro-inflammatory cytokines that are associated with an activated immune system can directly stimulate HIV replication. Progressive HIV disease and immune activation are therefore components of a positive feedback system in this way.
HIV disease –Immune activation –HIV disease –Immune activation
The process starts with HIV infection, and is promoted by other infections, some of which are activated by HIV infection. CMV has an important role in the process.
Whatever is driving immune activation is driving HIV disease.
I have tried to illustrate the positive feedback interactions with the following two diagrams.
Looking at the course of HIV infection in this way has a number of implications.
Pathogenesis.
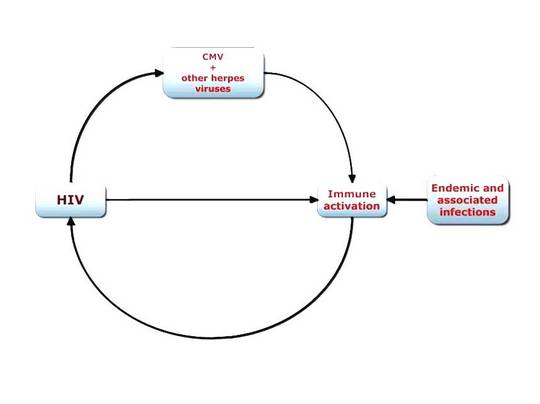
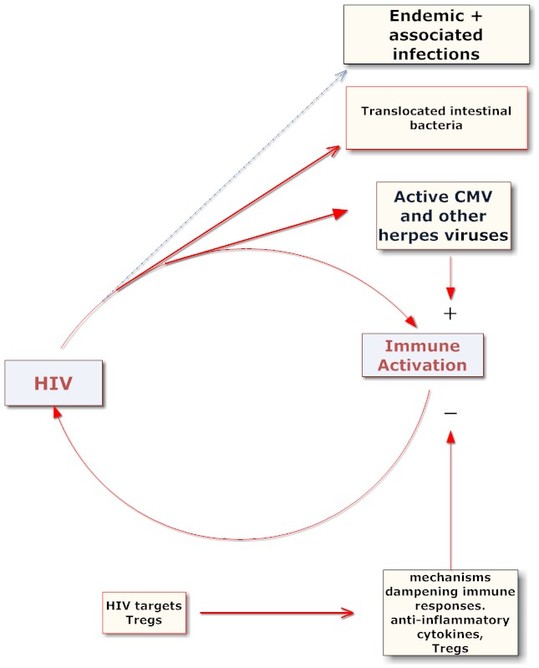
In the above diagram the course of HIV disease is represented by a potentially self perpetuating cycle proceeding in a clockwise direction. In addition to the elements that have positive effects in driving the process, there will also be those that retard the cycle. This is illustrated in the next diagram which focuses for simplicity on the immunological control of HIV infection and of those infections that add to immune activation. Of course there are other mitigating factors, for example, genetic factors conferring varying degrees of resistance to HIV resulting from receptor polymorphism.
In the diagram, the connection of HIV with CMV and other herpes viruses is probably constant and indicated by a red arrow. The connection of HIV with endemic and associated infections is indicated by a blue dotted line, because HIV infection does not increase susceptibility to all of them, nor does it accelerate the progression of all.

[ October 4, 2010: I have redrawn the above diagram.
See http://aidsperspective.net/blog/?p=584 for additional text]
The positive feedback cycle starts with HIV infection. At least some of the determinants of the rate of disease progression may be found in the conditions that exist at the time of initial infection that promote or retard the cycle.
There is evidence that the degree of immune activation at the time of seroconversion predicts future disease progression [12] [13] . It may also be an important determinant of what is called the set point. This is the point following initial infection with HIV, from which CD4 numbers decline.
The degree of immune activation at seroconversion influences the starting CD4 level; the rate of subsequent decline is influenced by the degree of immune activation in a system where once started, conditions can exist where immune activation increases with falling CD4 numbers, in a self perpetuating and accelerating fashion. Whatever the outcome, it will be the balance of positive and negative influences.
In the earliest years there were reports of EBV reactivation preceding HIV seroconversion [14] .
I have not seen any follow up of this interesting report. It at least suggests that there might even be situations in which active herpes infections can sometimes promote HIV seroconversion where HIV infection had only progressed to integration. They certainly produce signals that can activate HIV transcription from proviral DNA.
Treatment and prevention.
The role of immune activation in driving HIV disease is generally accepted now. There are sources of immune activation other than HIV and some of these can be controlled.
Attempts to identify and control additional sources of immune activation may be critical in the fight against HIV/AIDS.
Perhaps the most significant benefit in this respect concerns the developing world, where there are so many additional sources of immune activation that we are able to control. Even ascariasis, infestation with the common intestinal round worm is associated with significant immune activation. Worldwide prevalence is estimated to be about one billion, with 173 million in sub-Saharan Africa.
Many highly prevalent endemic infections can promote HIV replication. The control of these is a perfectly appropriate target in the fight against HIV/AIDS, and of course this would independently improve the lives of millions of individuals.
Measures to control endemic infections include traditional public health interventions, such as the provision of sanitation and clean water and the control of insect vectors. Effective drugs are sometimes inexpensive. Peter Hotez has written an article entitled “Africa’s 32 cent solution to AIDS” [15] . This refers to the price of Praziquantel , effective in treating schistosomiasis as a single dose.
The lives of impoverished populations are ravaged and shortened by these infections. Many of these infections also interact with HIV to compound the devastation they cause. Poverty, multiple endemic infections and HIV are intimately intertwined and in many instances reciprocally affect each other.
Recent and ongoing studies will probably lead to the routine use of drugs that are effective against herpesvirus infections. Trials of valacyclovir to reduce HIV viral loads are in progress. Given the ubiquitous nature of herpes infections, the use of acyclovir as adjunctive therapy might be warranted. Valacyclovir unfortunately is not yet available as a generic medication.
Unfortunately EBV and CMV are much more resistant to these drugs. The development of agents less toxic than valgancyclovir is important. Valgancyclovir has already been shown to reduce immune activation in HIV infected individuals as measured by a reduction in activated CD8 lymphocytes.
CMV is excreted in saliva, urine, and semen. Viral concentrations may be highest in semen. The unusual characteristic of CMV infection that enables the virus to infect an individual repeatedly has been described above. That it actually happens in the setting of HIV/AIDS was reported by Dr Drew in San Francisco in the late 1980s (something I had forgotten when writing a previous post).
In the late 1970s and early 1980s there was a high prevalence of CMV carriage in semen among gay men attending clinics for sexually transmitted infections. The following links are to some early papers that describe just how prevalent CMV excretion was among those individuals to be the first to show the abnormalities associated with HIV infection. I will just label these links with alphabet letters.
A (1981 report on prevalence of CMV infection); B ( indicates that semen is the main vehicle of transmission of CMV); C (CMV in HIV infected men); D (An article from Dr Drew in san Francisco on the efficacy of condoms in reducing CMV transmission); E (CMV detection in semen using PCR indicate a much higher rate of semen CMV carriage than noted previously with other detection methods)
Community viral load is a term that is now commonly used. By analogy I’d suggest the term “community CMV semen carriage”.
Condom use has almost surely reduced community CMV semen carriage. Condoms are effective in reducing CMV transmission. Reducing CMV transmission could have two effects. On an individual level, it’s possible that some increases in immune activation may be avoided. On a population level the reduction in community CMV semen carriage would be maintained or reduced even further.
Since CMV shedding increases with falling CD4 numbers it is of course likely that antiretroviral treatments will reduce CMV carriage in HIV infected individuals.
In summary it is useful to explicitly recognize the positive feedback interactions between HIV and many other infections. Prevention and treatment of those infections that contribute to immune activation and enhance HIV replication is absolutely relevant to the control of the HIV epidemic.




Comments
Comments