
The most recent revision of the DHHS guidelines on the use of antiretrovirals in adults and adolescents now recommends starting therapy at a CD4 lymphocyte count greater than 500/ mm3.,
This particular recommendation is unlike those made for individuals with lower CD4 numbers where more reliable evidence from clinical trials clearly demonstrates a benefit to the patient. For those with greater than 500 CD4 lymphocytes the recommendation is only supported by expert opinion - the opinions of the experts on the DHHS panel. There are plenty of other experts who are not so certain that starting treatment above 500 CD4 lymphocytes will confer a net benefit to the HIV infected individual.
Evidence based medicine has brought us a long way from the days when clinical decisions were based on authority and tradition (“expert opinion”); it attempts to use the best available evidence on which to base clinical recommendations. The term “best available evidence” means that not all types of evidence are of equal quality. There are several systems that grade the relative strengths of evidence derived from different sources. All agree that evidence provided by randomized controlled clinical trials is of the highest quality and therefore the most reliable. Applied to HIV medicine, a strong recommendation that antiviral treatment be initiated at 350 or fewer CD4s can be confidently made because the evidence of substantial benefit is derived from a randomized controlled clinical trial.
At the other end of the scale rating the quality of evidence, is evidence based on “expert opinion”. This may not even be a marginal improvement on the bad old days when the doctor knew best; when there was no need to justify a recommendation other than by the authority of the doctor or by tradition.
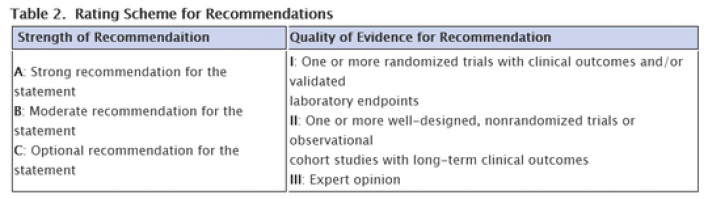
Here is the rating scheme used by the DHHS panel in making their treatment recommendations.
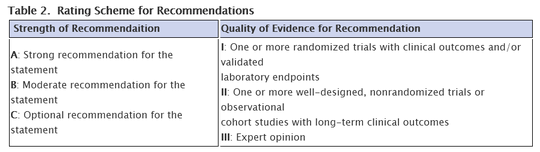
The rating of the recommendation that people with more than 500 CD4 lymphocytes start treatment is B III. It’s a moderate recommendation supported only by the opinion of experts.
But when expert opinion is the basis for a recommendation, this does not even mean that the opinion represents a consensus of all experts. It only represents the opinion of those experts chosen by the organization making the recommendation.
Making a recommendation based solely on expert opinion is particularly troublesome when the means exist to obtain evidence of the highest quality. The START trial that directly addresses the question of when it’s best to begin antiviral treatment is enrolling, and one must wonder why the panel did not defer making a recommendation concerning individuals with greater than 500 CD4 lymphocytes until the trial results become available. This is even more puzzling as individuals who have waited to start at CD4 numbers between 350 to 500 have in general done very well, so waiting to make a recommendation for some years until the START trial results are available seems to be a much more reasonable and prudent option than jumping the gun and making a recommendation based on evidence of the weakest quality.
Bur when we come to look at the associations of the experts on the DHHS panel, a recommendation based on expert opinion is even more problematic. We note that almost all of the non-governmental researchers have financial arrangements with entities that can benefit from the decisions they make. Some of these arrangements are quite extensive.
A conflict of interest becomes particularly troublesome when it’s only the opinion of the expert that supports a recommendation. Since people with greater than 500 CD4 lymphocytes represent a huge proportion of the HIV infected population, treating them will have an impact on expanding the market for antiviral drugs. With greater efforts to encourage testing, greater numbers of individuals with higher CD4 numbers will be identified, and now recommended to receive lifelong treatment with expensive and potentially toxic drugs whose benefits have not yet been proven to outweigh their harms.
Early AIDS activists performed a great service for all individuals who must deal with illness, in asserting their right to make informed decisions concerning their care, and that the decisions are made free from coercion. Withholding information and supplying misinformation are forms of coercion.
Although the guidelines ask physicians to inform patients with high CD4 numbers that evidence for benefit is not conclusive, I think it’s safe to conclude that individuals with greater than 500 CD4s will not always, and may only rarely be informed of this important caveat. As to informing patients of the conflicts of interest noted above, this isn’t even a consideration. They are also unlikely to be told that the recommendation that they start treatment is based on the opinion of certain experts only , and that there are other experts with a different opinion. In fact, the DHHS guidelines may be the only ones in the world to make this recommendation.
Undoubtedly the DHHS panel members believe that people with higher CD4 numbers will receive a net benefit from treatment. But the recommendations would have greater authority if the non-governmental researchers on the panel were better balanced with respect to members who had no financial arrangements with entities that stand to benefit from their decisions.
The recommendations also refer to the prevention benefit of treatment. The greatest prevention benefit will result from the treatment of individuals with lower CD4 numbers who will have the highest viral loads. These individuals need treatment. On this point there is no doubt or debate. For those with higher CD 4 numbers, not known at this time to benefit from treatment, the prevention benefit is likely to be much lower as their viral loads will also, on average be much lower than those with more advanced HIV disease.
Providing treatment to everybody who needs it should surely be our first priority. It is here that treatment will also have its greatest prevention benefit.
Two years ago in a tribute to Michael Callen I responded to similar recommendations to treat all HIV infected individuals irrespective of CD4 numbers.
I cannot express my reservations more clearly than with the words I used then:
I miss Michael Callen. He was my patient when AIDS began, but soon became my collaborator and friend.
For a time, Michael and Richard Berkowitz, another patient collaborator, were able to work out of an office adjoining my practice on W 12th street in New York City. It was in this setting that Michael and Richard learned about the medical aspects of this new disease and participated in the creation of some of the earliest organized community responses to the epidemic.
Michael and Richard helped in the formation of the AIDS Medical Foundation; they wrote the very first publication to recommend condom use by gay men. Michael played a role in the first attempt to protect the confidentiality of people with AIDS, and he helped to create both the Community Research Initiative and the PWA Health group.
A thread running through all of these endeavours is the notion of self empowerment. This extends beyond the belief that individuals who are fighting a disease should actively participate with their doctors in making decisions about the care they receive. Empowerment also means the inclusion of affected individuals at all levels of the response to the disease, from research to the provision of services.
The Community Research Initiative was sponsored by the PWA Coalition of which Michael was President. This is the very embodiment of self empowerment. It is people with a disease sponsoring research into that disease themselves and not waiting for some benevolent institution to come to the rescue.
Michael understood that his interests and priorities as a person living with AIDS might sometimes be at odds with those of some scientists conducting research into this new disease. He knew very well that he was living in a world that was still capable of cruel and discriminatory behavior towards him. Who better to protect the interests of those who had the most to lose than people living with AIDS themselves?
Self empowerment found expression in the Denver Principles. Michael and Richard were both signatories to this historic document. Michael played a major role in crafting the words of the Denver Principles.
Almost thirty years later these Principles remain as important as when they were first articulated.
One of the Denver principles asserts the right to obtain full explanations of all medical procedures and risks.
I wish Michael Callen were here today to bring attention to the violation of this right.
This is happening with little protest in places like San Francisco where antiviral medications are now recommended for healthier HIV positive individuals for whom the benefits of treatment have not been shown to outweigh the risks.
As always, you can’t beat the truth, and the truth is that for people with more than 350 CD4 lymphocytes, the best time to start treatment is not known. This may seem surprising as potent antiretroviral drugs have been available for fifteen years.
We have not yet done the kind of study that would most reliably provide the information those HIV positive individuals with higher CD4 numbers and their doctors need to make the best decisions about when to start treatment.
With information provided by a properly designed and conducted prospective randomized trial, we could know with confidence when in the course of HIV infection the benefits of treatment absolutely outweigh the risks.
Some feel that a decision can be made with less reliable information. But surely all would agree that a decision to start treatment or to defer it must always be an informed one voluntarily made by the individual considering treatment.
It is here that the principle asserting the right to a full explanation of the risks of medical interventions is being violated.
The San Francisco Department of Public Health in advising all HIV infected individuals to receive treatment is in effect telling them that at all stages of HIV disease the benefits of treatment outweigh the risks. This may be so, but apart from those with 350 or fewer CD4 lymphocytes, we just do not have the most reliable evidence to support this contention.
People with higher CD4 numbers have the right to know not only what evidence there is that immediate treatment will have a net benefit compared to deferring it, but also the quality of that evidence. They surely should also be made aware that experts hold differing opinions on whether treatment should begin immediately or be deferred.
A physician in San Francisco who recommended that all HIV infected individuals should start treatment immediately was reported to have said:
“If I’m wrong, we’ll start people [on treatment] a couple years earlier than we otherwise would. But if I’m right and we don’t start early, there’s no going back,”
Others who are concerned about drug side effects might feel that more may be at stake for HIV positive individuals with higher CD4 numbers. This also includes the possibility that fewer options may be available when treatment is definitely known to be needed.
This doctor is also reported to have said:
“The old paradigm was that drugs are toxic so we should wait as long as possible. The new paradigm is that while today’s drugs are not totally benign, they are less toxic than the virus.”
“The” paradigm? Is it not misleading to give an impression that his views on drug toxicities represent a consensus?
How on earth can the longer term toxicities of the newer drugs be known?
Just a few days ago it was reported that AZT and 3TC based therapies produced a metabolic abnormality called hyperhomocysteinemia. This is a condition associated with vascular abnormalities including a greatly higher risk of heart attacks. We have been prescribing AZT and 3TC for about twenty years, so what information does the San Francisco doctor have that gives him such confidence that the drugs in use for only a few years are less toxic?
Empowerment means that HIV positive individuals make their own decisions to start or to defer treatment. They have the right to clear and honest information to enable them to make this decision. Those with higher CD4 counts have the right to know that there still is uncertainty about when it is best to start treatment.
The views of the San Francisco Department of Public health and those who share them are just opinions; healthier HIV positive individuals should also know that these opinions are not held by all experts. Respect for the autonomy of healthier HIV positive individuals requires that opposing views on when it’s best to start treatment be presented together with the evidence supporting these views, so those who have most at stake can decide for themselves.
There will continue to be opposing views on when it’s best to start antiviral therapy as long as the question has not been put to the test.
The best way to resolve uncertainty in clinical medicine is by conducting prospective randomized trials. A properly designed and conducted trial could reliably and safely answer the question of whether, on average, immediate or deferred treatment is better or worse or makes no difference.
HIV positive individuals deserve the most reliable information to inform them in making treatment decisions. The START trial is a randomized prospective study that directly asks the question about the best time to start antiviral medications. We could really finally know what’s best, and no longer rely on opinions based on data of inferior quality.
Is an immediate or deferred initiation of treatment better or worse, or does it make no difference? If knowledge is power a demand to complete the START trial is the embodiment of the self empowerment of HIV positive individuals. The very antithesis of self empowerment is to allow researchers to persuade us with evidence of inferior quality, such as their personal opinions, presented as if there were a consensus, or with the results of embarrassingly uninterpretable studies such as NA-ACCORD so often used to justify earlier starts to treatment. NA-ACCORD was not a prospective randomized trial. It was a review of a large number of medical records. Such retrospective observational studies are beset with interpretative difficulties because subjects are not randomly assigned to receive one or another kind of intervention, in this case, to start treatment early or to defer it. We don’t know why a particular course of action was chosen. The reasons why decisions were made to start treatment early or to defer it may have determined the outcome rather than the time treatment was started.
In situations where prospective randomized trials cannot be conducted for whatever reasons, then we have to do the best with data of inferior quality. But fortunately this is not the case with HIV infection.
I miss Michael Callen. He would have reminded us that HIV positive individuals must demand that the best evidence be obtained to inform their treatment choices.




5 Comments
5 Comments